CONTINUING PROFESSIONAL DEVELOPMENT FOR NURSES
FREE! Stop That Clot: Haemostasis and anticoagulants
2 hours
2 hours
Prevention of haemostasis
Intact endothelium produces heparan sulphate (similar to heparin) which combines with, and activates, antithrombin (AT) in plasma (Tanaka et al., 2009). AT inactivates many clotting factors particularly Xa and thrombin. Other endothelial products e.g. prostaglandins and nitric oxide inhibit platelet activation. Proteins C and S are anticoagulant factors found in the plasma that also inhibit clotting (Rang et al., 2012) All of these molecules act to prevent abnormal clotting or extension of clots beyond an area of damage.The ability of endothelium to produce these inhibitory substances is affected by direct damage and by the presence of inflammatory or tumour-promoting chemicals in the blood.
Any of these may be sufficient to cause thrombosis but risk increases with the number of factors present. Consequences of thrombus formation depend on whether it forms in an artery or vein, and on the particular vessel in which it occurs.
Thrombus Formation
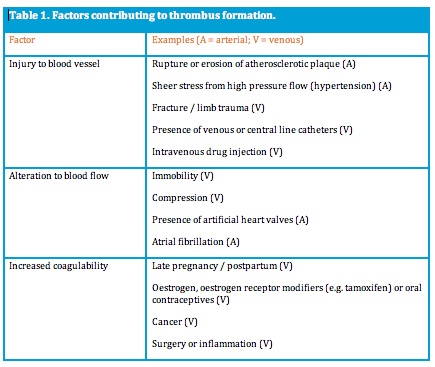
Thrombosis is an abnormal activation of haemostatic mechanisms that may lead to occlusion of a vessel and/or to development of an embolus that travels and obstructs a smaller vessel. Precipitating factors for thrombosis are injury to a blood vessel, stasis or alteration to blood flow, and increased coagulability of blood (Table 1).Any of these may be sufficient to cause thrombosis but risk increases with the number of factors present. Consequences of thrombus formation depend on whether it forms in an artery or vein, and on the particular vessel in which it occurs.
Venous Thromboembolism (VTE)
Deep vein thrombosis (DVT) most often occurs in veins of the upper and lower leg. Incidence, without prophylactic therapy, is around 50% of patients hospitalised for stroke or orthopaedic surgery (Australian and New Zealand Working Party on the Management and Prevention of Thromboembolism, 2007). In the UK, it is estimated that hospital acquired, preventable VTE causes 25,000 deaths each year (NICE, 2013). In pregnancy and postpartum, VTE accounts for 10 per cent of maternal deaths, with a 20-fold increase in risk for DVT postpartum compared to non pregnant women (James, 2009).Many venous thrombi are asymptomatic. Adverse outcomes for DVT include pulmonary embolism, chronic venous insufficiency and a high risk of recurrence. Pulmonary embolism accounts for approximately 9% of all hospital deaths (Ruppert et al., 2010) and, with survival, there is increased risk of chronic pulmonary hypertension.
Diagnosis of DVT relies on presence of risk factors, probability factors (tenderness, swelling, oedema and presence of visible superficial veins in the affected limb), and the absence of other likely causes (The Merck Manual, 2009; NICE, 2012). This information can be used to provide a score of suspicion - the Two level DVT Wells score - which then indicates the need for further investigation (NICE, 2012).
Diagnosis of DVT relies on presence of risk factors, probability factors (tenderness, swelling, oedema and presence of visible superficial veins in the affected limb), and the absence of other likely causes (The Merck Manual, 2009; NICE, 2012). This information can be used to provide a score of suspicion - the Two level DVT Wells score - which then indicates the need for further investigation (NICE, 2012).
D-dimer blood testing may be performed. D-dimer is a fragment of fibrin that indicates recent clot formation and lysis. D-dimer tests are not specific to DVT and are not considered a reliable diagnostic tool, but a normal D-dimer result may denote absence of DVT (The Merck Manual, 2009; NICE, 2012). Ultrasound is the most accurate way of determining presence of a DVT.
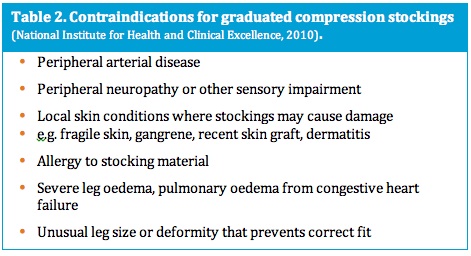
Prophylaxis of VTE reduces mortality and morbidity. The use of graduated compression stockings (GCS) for all at risk patients is increasingly common and supported by research, although stockings are commonly used in conjunction with antithrombotic medication (NHMRC, 2009). GCS reduce venous dilation, increasing rate of blood flow and increasing efficiency of valves in the walls of veins. Risk of DVT can be reduced by 51% using GCS (Phillips et al., 2008). Patients must be assessed for appropriate use of GCS, including contraindications (Table 2), and measured to ensure proper fit (NICE, 2010).
Those at higher risk of VTE may have intermittent pneumatic compression or venous foot pump therapy while immobilised. All mechanical forms of prophylxis reduce venous stasis and/or increase venous outflow from the leg (Geerts, et al., 2008).
Drugs for prophylaxis of VTE include low dose unfractionated heparin (UFH) and low molecular weight heparins (LMWH) such as enoxaparin, or rivaroxiban, an oral factor Xa inhibitor. These drugs are used in treatment of established VTE along with warfarin. None of these drugs dissolves established clots: they stabilise and prevent extension of existing thrombi, reducing risk of emboli.
Prophylaxis of VTE reduces mortality and morbidity. The use of graduated compression stockings (GCS) for all at risk patients is increasingly common and supported by research, although stockings are commonly used in conjunction with antithrombotic medication (NHMRC, 2009). GCS reduce venous dilation, increasing rate of blood flow and increasing efficiency of valves in the walls of veins. Risk of DVT can be reduced by 51% using GCS (Phillips et al., 2008). Patients must be assessed for appropriate use of GCS, including contraindications (Table 2), and measured to ensure proper fit (NICE, 2010).
Those at higher risk of VTE may have intermittent pneumatic compression or venous foot pump therapy while immobilised. All mechanical forms of prophylxis reduce venous stasis and/or increase venous outflow from the leg (Geerts, et al., 2008).
Drugs for prophylaxis of VTE include low dose unfractionated heparin (UFH) and low molecular weight heparins (LMWH) such as enoxaparin, or rivaroxiban, an oral factor Xa inhibitor. These drugs are used in treatment of established VTE along with warfarin. None of these drugs dissolves established clots: they stabilise and prevent extension of existing thrombi, reducing risk of emboli.





